
How many days a month does a person actually expect to want this?
That single question, more than any drug trial, is what decides between sildenafil and tadalafil. Both are proven. Both are first-line. The molecule that fits is the one that matches the rhythm of a life, not the one with better brand recognition. Here is the case laid out question by question.
What do the two drugs actually have in common?
Quite a lot, and it matters to say so before getting into the differences. Sildenafil is the molecule sold as Viagra. Tadalafil is the one sold as Cialis. Both belong to the same drug class, PDE5 inhibitors, and both are named by the American Urological Association guideline as first-line oral therapy for erectile dysfunction [1]. Both work by blocking the enzyme that breaks down cyclic GMP. With that enzyme out of the way, cyclic GMP builds up, vascular smooth muscle relaxes, and blood flow increases [2]. Both are available as FDA-approved generics. Both carry the same class of mild, temporary side effects, things like headache, flushing, nasal congestion [2]. And both carry one identical, serious warning, addressed further down, that outranks every other consideration in this comparison. On raw effectiveness, for the right candidate, neither one beats the other in the literature. The split shows up somewhere else entirely.
Where do they actually split?
Timing. That is nearly the whole story.
Sildenafil is built for occasional use. Someone takes it ahead of activity, it does its work for a window of hours, then it clears, with the reference literature framing the relevant nitrate-safety horizon at roughly 24 hours [2]. That suits a person who would rather take a pill only when a pill is wanted, and otherwise take nothing at all.
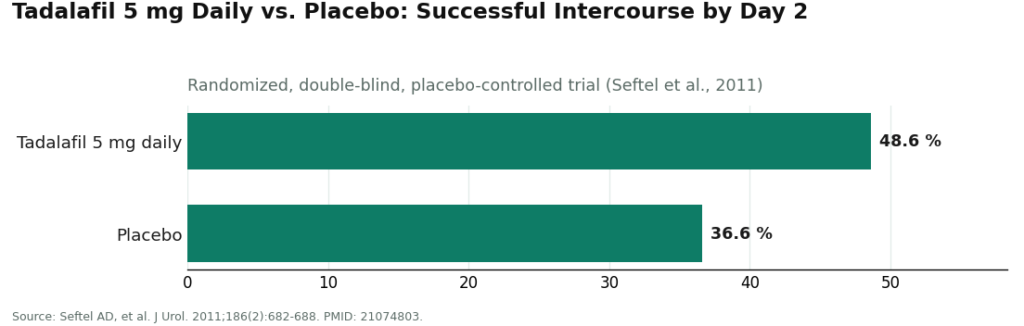
Tadalafil’s defining trait is duration. It lasts long enough to support a second strategy sildenafil cannot really offer: a low dose, taken every day, so the drug is simply always on board and nobody has to plan sex around a pill. A randomized, double-blind, placebo-controlled trial tested tadalafil 5 mg once daily and found significantly more men reporting successful intercourse than those on placebo by day two, 48.6 percent versus 36.6 percent [4]. That gap is the whole argument for the daily approach in one number.
Is daily tadalafil actually backed by evidence, or is that just how it’s marketed?
Backed by evidence, and the direction of the finding is a little counterintuitive. A meta-analysis in the journal Sexual Medicine pooled long-term data, at least 24 weeks, comparing daily tadalafil against on-demand tadalafil. It found the daily regimen gave a better therapeutic effect and fewer treatment-emergent adverse events than dosing only as needed [3]. Most people would guess that taking a pill every day means more side effects than taking it occasionally. This body of pooled evidence says otherwise, at least across the populations studied. One caveat belongs here: a meta-analysis averages across different studies and different men. It describes a trend, not a promise for any one person.
So which strategy fits which life?
Three scenarios cover most people, and each maps to a different answer.
Wants sex occasionally, dislikes the idea of a standing prescription. On-demand sildenafil is built for exactly this. Take it, use it, done, nothing in the system the rest of the month.
Wants spontaneity, doesn’t want to think about timing at all. Daily low-dose tadalafil is the tool designed for this, and the meta-analysis above says it holds up well over the long run [3].
Cares about total drug exposure over time. This is a genuine tradeoff, not a false choice. On-demand dosing means less cumulative medication across a month. Daily dosing means more, traded for constant readiness. Neither answer is wrong; it depends what a person values.
Notice what’s missing from that list: a specific milligram number to self-select. The 5 mg daily figure above is the dose that was studied, offered here as evidence, not as an instruction. What dose, and whether either drug is appropriate at all, is a determination a clinician makes after reviewing the whole picture, not a number a reader picks off a page.
Is there a risk that overrides all of this?
Yes, and it isn’t close. Both sildenafil and tadalafil, being PDE5 inhibitors, can cause a severe, life-threatening drop in blood pressure when combined with nitrate medications. The clinical reference is blunt about it: coadministration with nitrates is contraindicated, and nitrate use is only considered safe once the drug has cleared the system, on the order of 24 hours for sildenafil, with tadalafil’s longer action carrying its own clearance window [2]. Nitrates are common heart medications, frequently prescribed for angina, and the population asking about ED treatment overlaps heavily with the population that might already be on one. For anyone taking a nitrate, this whole comparison is on hold until a clinician has looked at the interaction. Sildenafil versus tadalafil is the second question. The nitrate check is the first.
There’s a related reason ED deserves a real look rather than a quick prescription: it’s frequently an early signal of cardiovascular disease, and the AUA guideline says patients should be counseled on that basis [1]. The same cardiovascular thread that makes the nitrate question urgent is the reason the visit itself should be a genuine evaluation.
Does it matter which online clinic runs that evaluation?
It does, because the whole comparison above is only as good as the intake behind it. A 2023 analysis in Sexual Medicine looked at 15 direct-to-consumer ED platforms. Fourteen of them opened with nothing more than an online form. Only four explicitly advertised that a physician would actually handle the consultation. And the cardiovascular link the AUA guideline emphasizes was, in the study authors’ own words, “unlikely to be addressed” [5]. Put plainly: the same visit that’s supposed to pick sildenafil or tadalafil is the visit that’s supposed to catch the nitrate risk and flag a possible cardiovascular warning sign. If that visit is thin, both jobs go undone.
This is why a supervised-access structure isn’t a side note to this comparison, it’s load-bearing. A model where a licensed clinician reviews the case before anything is prescribed, and a licensed pharmacy fills it, is what turns “which drug fits my goal” into an actual medical decision instead of a shopping choice. FormBlends builds its process on that footing: a clinician reviews each request before a prescription is written, and licensed pharmacies handle the fill. That’s a description of how the process is structured, nothing more, no cart, nothing for sale here.
What’s the short version?
Sildenafil and tadalafil are both well-evidenced, both first-line, and both work the same way, so the real decision isn’t which is stronger, it’s which dosing rhythm fits a life. Sildenafil suits planned, occasional use. Tadalafil’s longer action opens up a daily low-dose option that the pooled long-term evidence backs as effective and well tolerated [3][4]. Total drug exposure is the honest tradeoff between the two. And none of it applies until the nitrate contraindication has been ruled out and a real evaluation, of the kind the guideline and the cardiovascular research both call for, has actually happened [1][2].
Questions people actually ask
Is sildenafil or tadalafil more effective for erectile dysfunction? Neither has a categorical edge for someone who’s a good candidate. Both are named first-line by the AUA guideline, and controlled trials back each one [1]. The real difference is timing, not strength, so the “better” drug is whichever one’s schedule matches the person taking it.
Why does tadalafil’s longer duration matter so much? Because it enables daily low-dose use, which keeps the drug present at all times and removes the need to time a pill around sex. In a randomized, double-blind, placebo-controlled trial, tadalafil 5 mg once daily produced significantly more successful-intercourse reports than placebo by day two, 48.6 percent versus 36.6 percent [4]. Sildenafil’s shorter window is built for planned, occasional use instead.
Is daily tadalafil actually better than taking it only when needed? According to a meta-analysis in Sexual Medicine pooling long-term data over at least 24 weeks, yes: the daily regimen showed a better therapeutic effect and fewer treatment-emergent side effects than on-demand dosing [3]. That cuts against the assumption that daily dosing means more side effects. It’s a pooled average across varied studies, though, not a guaranteed individual result.
Can either drug be combined with nitrate medications? No. Combining a PDE5 inhibitor with nitrates can cause a severe, life-threatening blood pressure drop, and the drug reference treats it as a flat contraindication [2]. Nitrates are considered safe only once the drug has cleared, roughly 24 hours for sildenafil, with tadalafil requiring its own longer clearance window. Because nitrates are common heart medications, this interaction outranks any preference between the two drugs until it’s been checked.
Does the online clinic actually change the outcome, or is it just paperwork? It changes the outcome, because the drug choice is only as sound as the visit behind it. A 2023 review of 15 direct-to-consumer ED platforms found 14 opened with just an intake form, only 4 advertised an actual physician consultation, and the cardiovascular link the guideline stresses was, per the authors, “unlikely to be addressed” [5]. The same evaluation that picks a drug also has to catch the nitrate risk and the cardiovascular red flag ED can represent.
How does an online ED clinic actually work?
A questionnaire comes first, then a licensed physician or nurse practitioner reviews it, and if things check out, a prescription goes to a pharmacy. Most intakes run under 20 minutes. Some platforms review answers asynchronously, on the provider’s own schedule; others offer a short live video call. Either way, the prescribing call belongs to a real clinician, not an algorithm.
What does an online ED clinic typically cost, and what moves the price?
Consultation fees range from free up to about $50, depending on the platform, and generic sildenafil can run as low as $1 to $3 per pill when bought in bulk. Branded drugs, newer formulations, and compounded doses cost more. Subscriptions sometimes lower the per-pill price in exchange for locking a person into regular shipments. Worth checking whether a quoted price covers the pharmacy fill or only the visit.
Is it actually safe to get ED medication through an online clinic?
It’s safe when the platform uses state-licensed prescribers and fills through licensed pharmacies. The danger sits with sites that skip the clinical review or source drugs outside regulated supply chains. Sildenafil and tadalafil carry real contraindications, nitrates especially, so a genuine medical review isn’t optional. Compounding pharmacies working under physician supervision, FormBlends among them, sit in a legitimate, accountable tier for cases where standard doses don’t fit.
How does someone actually get started with an online ED clinic?
Choose a platform that clearly names its prescribers and pharmacy partners, then fill out the intake honestly, heart medications and blood pressure drugs included. Have pharmacy details ready in case the prescription gets sent there rather than filled in-house. Most people get a prescribing decision within hours. If the questionnaire never asks about cardiovascular history, that’s a red flag worth taking seriously.
References
- Erectile Dysfunction: AUA Guideline. American Urological Association (Burnett AL, et al.), published 2018, amended through 2018. Names FDA-approved oral PDE5 inhibitors (sildenafil, tadalafil, vardenafil, avanafil) as first-line therapy unless contraindicated and identifies ED as a risk marker for cardiovascular disease warranting patient counseling. https://www.auanet.org/guidelines-and-quality/guidelines/erectile-dysfunction-(ed)-guideline
- Smith BP, Babos M. Sildenafil. StatPearls. NCBI Bookshelf (NBK558978). Describes the PDE5 inhibitor mechanism (inhibition of cGMP degradation), the generally mild vasodilatory side-effect class, and states that coadministration with nitrates is contraindicated because the combination can cause severe, life-threatening hypotension, with nitrate use considered safe only after roughly 24 hours for sildenafil. https://www.ncbi.nlm.nih.gov/books/NBK558978/
- Zhou Z, Chen H, Wu J, Wang J, Zhang X, Ma J, Cui Y. Meta-Analysis of the Long-Term Efficacy and Tolerance of Tadalafil Daily Compared With Tadalafil On-Demand in Treating Men With Erectile Dysfunction. Sex Med. 2019;7(3):282-291. DOI: 10.1016/j.esxm.2019.06.006. Concluded tadalafil daily provides a preferable therapeutic effect with a lower incidence of treatment-emergent adverse events relative to on-demand dosing over at least 24 weeks.
- Seftel AD, Goldfischer E, Kim ED, Dula E, Zeigler H, Burns P. Onset of efficacy of tadalafil once daily in men with erectile dysfunction: a randomized, double-blind, placebo controlled trial. J Urol. 2011;186(2):682-688. PMID: 21074803. Used tadalafil 5 mg once daily; significantly more men achieved successful intercourse than those on placebo by day 2 (48.6% vs 36.6%, p < 0.025).
- Brink SM, Iarajuli T, Shin D. Characteristics of direct-to-consumer platforms offering erectile dysfunction treatment. Sex Med. 2023;11(4):qfad038. PMID: 37547870; PMCID: PMC10397420. Of 15 DTC platforms, 14 (93%) began with an online intake form and only 4 (27%) explicitly advertised physician consultation; the ED-cardiovascular link “was unlikely to be addressed.”
Written by Vera Cho, wellness reporter. Last reviewed May 2026.
This is general reference material, not personalized medical advice. Loop in a licensed clinician first.



